Acute respiratory infection (ARI) is a leading cause of morbidity and mortality in children in low and middle-income countries. Human metapneumovirus (HMPV) is a common virus associated with acute lower respiratory infections (ALRIs) in children. We aimed to estimate the global prevalence, hospital admissions, and clinical complications of HMPV-associated ALRI in children. Between 2005 and 2024, we estimated the global burden of human metapneumovirus-associated ALRIs in children from more than 30 studies. We included data for any length of study period. We included data on the proportion of HMPV-positive cases among hospitalized ALRI cases and patient attending outdoor wings with complain of severe or mild respiratory complications. According to estimates, HMPV caused 14.2 million ALRI cases in children under the age of five in 2018, which resulted in 643,000 hospital admissions and 7,700 in-hospital deaths. Children hospitalized with HMPV infection, as compared with those hospitalized without HMPV infection, were older and more likely to receive a diagnosis of pneumonia or asthma, to require supplemental oxygen, and to have a longer stay in the intensive care unit. Fever (97%) and cough (96%) were the most common presenting symptoms of HMPV-associated pneumonia and were also common symptoms of other pathogens. This study describes global prevalence and clinical complications of HMPV associated ALRIs in children. Clinical features did not reliably distinguish HMPV-associated ALRI from other respiratory infections.
| Published in | International Journal of Infectious Diseases and Therapy (Volume 10, Issue 2) |
| DOI | 10.11648/j.ijidt.20251002.12 |
| Page(s) | 39-46 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Human Metapneumovirus (HMPV), Acute Lower Respiratory Infections (ALRIs), Global Burden, Pneumonia
Characteristics | Inpatients | Outpatients | ||||
|---|---|---|---|---|---|---|
HMPV-Positive (N=200) | HMPV-Negative (N=3290) | P value | HMPV-Positive (N=446) | HMPV-Negative (N=5812) | P value | |
Age- m | ||||||
Median | 13 | 6 | <0.001 | 17 | 16 | 0.61 |
Interquartile range | 5-26 | 1-19 | 8-32 | 8-32 | ||
Age group | <0.001 | 0.59 | ||||
<6 m | 56 (28%) | 1614 (49%) | 71 (16%) | 1036 (18%) | ||
6-11m | 39 (20%) | 443 (13%) | 96 (22%) | 1148 (20%) | ||
12-23m | 49 (24%) | 605 (18%) | 114 (26%) | 1524 (26%) | ||
24-35m | 27 (14%) | 291 (9%) | 77 (17%) | 892 (15%) | ||
36-54m | 29 (14%) | 337 (10%) | 88 (20%) | 1212 (21%) | ||
Sex | 0.16 | 0.35 | ||||
Male | 105 (52%) | 1892 (58%) | 248 (56%) | 3099 (53%) | ||
Female | 95 (48%) | 1398 (42%) | 198 (44%) | 2713 (47%) | ||
High-risk condition | 81 (40%) | 990 (30%) | 0.002 | 0.81 | ||
Premature birth | 48 (24%) | 513 (16%) | 0.006 | 39 (9%) | 585 (10%) | 0.34 |
Asthma | 61 (30%) | 677 (21%) | <0.001 | 83 (19%) | 1084 (18%) | 0.98 |
Chronic Lung disease | 20 (10%) | 182 (6%) | 0.009 | 1 (<1) | 70 (1%) | 0.06 |
Supplemental oxygen | 106 (53%) | 1178 (36%) | <0.001 | - | - | |
HMPV | Human Metapneumovirus |
ALRI | Acute Lower Respiratory Infection |
IPD | Inpatient Department |
OPD | Outdoor Patient Department |
ED | Emergency Department |
RSV | Respiratory Syncytial Virus |
| [1] | Widmer, K., Griffin, M. R., Zhu, Y., Williams, J. V., & Talbot, H. K. (2014). Respiratory syncytial virus‐and human metapneumovirus-associated emergency department and hospital burden in adults. Influenza and other respiratory viruses, 8(3), 347-352. |
| [2] | Caracciolo, S., Minini, C., Colombrita, D., Rossi, D., Miglietti, N., Vettore, E.,... & Fiorentini, S. (2008). Human metapneumovirus infection in young children hospitalized with acute respiratory tract disease: virologic and clinical features. The Pediatric infectious disease journal, 27(5), 406-412. |
| [3] | Al Mamun, A., & Hapsari, R. N. W. (2025). Human Metapneumovirus (HMPV) Outbreaks in Focus: A call for Preparedness and Action. Health Dynamics, 2(1), 1-3. |
| [4] | Shafagati, N., & Williams, J. (2018). Human metapneumovirus-what we know now. F1000 Research, 7, 135. |
| [5] | Rahman, M. Z., Sumiya, M., Sahabuddin, M., Pell, L. G., Gubbay, J. B., Rahman, R., & Morris, S. K. (2019). Genetic characterization of human metapneumovirus identified through community and facility-based surveillance of infants in Dhaka, Bangladesh. Journal of Medical Virology, 91(4), 549-554. |
| [6] | Feuillet, F., Lina, B., Rosa-Calatrava, M., & Boivin, G. (2012). Ten years of human metapneumovirus research. Journal of clinical virology, 53(2), 97-105. |
| [7] | Haas, L. E., Thijsen, S. F., Van Elden, L., & Heemstra, K. A. (2013). Human metapneumovirus in adults. Viruses, 5(1), 87-110. |
| [8] | Williams, J. V., Edwards, K. M., Weinberg, G. A., Griffin, M. R., Hall, C. B., Zhu, Y., & Crowe Jr, J. E. (2010). Population-based incidence of human metapneumovirus infection among hospitalized children. The Journal of infectious diseases, 201(12), 1890-1898. |
| [9] | Yang, C. F., Wang, C. K., Tollefson, S. J., Piyaratna, R., Lintao, L. D., Chu, M., & Williams, J. V. (2009). Genetic diversity and evolution of human metapneumovirus fusion protein over twenty years. Virology journal, 6, 1-10. |
| [10] | Kulkarni, D., Cong, B., Ranjini, M. J. K., Balchandani, G., Chen, S., Liang, J., & Nair, H. (2025). The global burden of human metapneumovirus-associated acute respiratory infections in older adults: a systematic review and meta-analysis. The Lancet Healthy Longevity. |
| [11] | del Valle-Mendoza, J., Orellana-Peralta, F., Del Valle, L. J., Verne, E., Ugarte, C., Weilg, C., & Aguilar-Luis, M. A. (2019). Detection of human Metapneumovirus infection in children under 18 years old hospitalized in Lima-Peru. PeerJ, 7, e7266. |
| [12] | Amer, H. M. (2016). Molecular epidemiology of human metapneumovirus in Riyadh Province, Saudi Arabia. Journal of Molecular Microbiology and Biotechnology, 26(6), 414-421. |
| [13] | Xiao, N. G., Zhang, B., Xie, Z. P., Zhou, Q. H., Zhang, R. F., Zhong, L. L., & Duan, Z. J. (2013). Prevalence of human metapneumovirus in children with acute lower respiratory infection in Changsha, China. Journal of medical virology, 85(3), 546-553. |
| [14] | Yelamanchili, S., Gujjarlapudi, D., Chella, N., Dulla, V. R., & Duvvur, N. R. (2025). Human Metapneumovirus seroprevalence and PCR trends-Findings from a Tertiary Care Hospital in India. medRxiv, 2025-02. |
| [15] | Haynes, A. K., Fowlkes, A. L., Schneider, E., Mutuc, J. D., Armstrong, G. L., & Gerber, S. I. (2016). Human metapneumovirus circulation in the United States, 2008 to 2014. Pediatrics, 137(5). |
| [16] | Anjorin, A. A. A., Olaleye, H. O., Sayid, S. A., Ajose, T. D., Daniel, G. T., & Akinyemi, K. O. (2025). Molecular Detection of Human Metapneumovirus in Lagos, Nigeria. medRxiv, 2025-02. |
| [17] | Neemuchwala, A., Duvvuri, V. R., Marchand-Austin, A., Li, A., & Gubbay, J. B. (2015). Human metapneumovirus prevalence and molecular epidemiology in respiratory outbreaks in Ontario, Canada. Journal of medical virology, 87(2), 269-274. |
| [18] | Vinomarlini, G., Samuel, L., Thayan, R., Zainah, S., & Bhassu, S. (2014). Incidence of Human Metapneumovirus in Hospitalized Patients Admitted for Respiratory Illness in Malaysia. Int Res J Biological Sci, 3, 51-7. |
| [19] | Van den Hoogen, B. G., Herfst, S., Sprong, L., Cane, P. A., Forleo-Neto, E., De Swart, R. L., & Fouchier, R. A. (2004). Antigenic and genetic variability of human metapneumoviruses. Emerging infectious diseases, 10(4), 658. |
| [20] | Edwards, K. M., Zhu, Y., Griffin, M. R., Weinberg, G. A., Hall, C. B., Szilagyi, P. G., & Williams, J. V. (2013). Burden of human metapneumovirus infection in young children. New England Journal of Medicine, 368(7), 633-643. |
| [21] | Gaunt, E., McWilliam-Leitch, E. C., Templeton, K., & Simmonds, P. (2009). Incidence, molecular epidemiology and clinical presentations of human metapneumovirus; assessment of its importance as a diagnostic screening target. Journal of clinical virology, 46(4), 318-324. |
| [22] | Wang, X., Li, Y., Deloria-Knoll, M., Madhi, S. A., Cohen, C., Ali, A., & Morpeth, S. (2021). Global burden of acute lower respiratory infection associated with human metapneumovirus in children under 5 years in 2018: a systematic review and modelling study. The Lancet Global Health, 9(1), e33-e43. |
| [23] | Howard, L. M., Edwards, K. M., Zhu, Y., Grijalva, C. G., Self, W. H., Jain, S., & Williams, D. J. (2021). Clinical features of human metapneumovirus-associated community-acquired pneumonia hospitalizations. Clinical Infectious Diseases, 72(1), 108-117. |
| [24] | Panda, S., Mohakud, N. K., Pena, L., & Kumar, S. (2014). Human metapneumovirus: review of an important respiratory pathogen. International journal of infectious diseases, 25, 45-52. |
| [25] | Wang, X., Li, Y., O'brien, K. L., Madhi, S. A., Widdowson, M. A., Byass, P.,... & Schweiger, B. (2020). Global burden of respiratory infections associated with seasonal influenza in children under 5 years in 2018: a systematic review and modelling study. The Lancet Global Health, 8(4), e497-e510. |
APA Style
Ahmed, S. N., Mukharjee, D., Akhter, S. (2025). Global Burden and Clinical Complications of Human Metapneumovirus Associated with Acute Lower Respiratory Infection in Children: A Short Review. International Journal of Infectious Diseases and Therapy, 10(2), 39-46. https://doi.org/10.11648/j.ijidt.20251002.12
ACS Style
Ahmed, S. N.; Mukharjee, D.; Akhter, S. Global Burden and Clinical Complications of Human Metapneumovirus Associated with Acute Lower Respiratory Infection in Children: A Short Review. Int. J. Infect. Dis. Ther. 2025, 10(2), 39-46. doi: 10.11648/j.ijidt.20251002.12
AMA Style
Ahmed SN, Mukharjee D, Akhter S. Global Burden and Clinical Complications of Human Metapneumovirus Associated with Acute Lower Respiratory Infection in Children: A Short Review. Int J Infect Dis Ther. 2025;10(2):39-46. doi: 10.11648/j.ijidt.20251002.12
@article{10.11648/j.ijidt.20251002.12,
author = {Shamsun Nahar Ahmed and DebJyoti Mukharjee and Shameem Akhter},
title = {Global Burden and Clinical Complications of Human Metapneumovirus Associated with Acute Lower Respiratory Infection in Children: A Short Review
},
journal = {International Journal of Infectious Diseases and Therapy},
volume = {10},
number = {2},
pages = {39-46},
doi = {10.11648/j.ijidt.20251002.12},
url = {https://doi.org/10.11648/j.ijidt.20251002.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijidt.20251002.12},
abstract = {Acute respiratory infection (ARI) is a leading cause of morbidity and mortality in children in low and middle-income countries. Human metapneumovirus (HMPV) is a common virus associated with acute lower respiratory infections (ALRIs) in children. We aimed to estimate the global prevalence, hospital admissions, and clinical complications of HMPV-associated ALRI in children. Between 2005 and 2024, we estimated the global burden of human metapneumovirus-associated ALRIs in children from more than 30 studies. We included data for any length of study period. We included data on the proportion of HMPV-positive cases among hospitalized ALRI cases and patient attending outdoor wings with complain of severe or mild respiratory complications. According to estimates, HMPV caused 14.2 million ALRI cases in children under the age of five in 2018, which resulted in 643,000 hospital admissions and 7,700 in-hospital deaths. Children hospitalized with HMPV infection, as compared with those hospitalized without HMPV infection, were older and more likely to receive a diagnosis of pneumonia or asthma, to require supplemental oxygen, and to have a longer stay in the intensive care unit. Fever (97%) and cough (96%) were the most common presenting symptoms of HMPV-associated pneumonia and were also common symptoms of other pathogens. This study describes global prevalence and clinical complications of HMPV associated ALRIs in children. Clinical features did not reliably distinguish HMPV-associated ALRI from other respiratory infections.
},
year = {2025}
}
TY - JOUR T1 - Global Burden and Clinical Complications of Human Metapneumovirus Associated with Acute Lower Respiratory Infection in Children: A Short Review AU - Shamsun Nahar Ahmed AU - DebJyoti Mukharjee AU - Shameem Akhter Y1 - 2025/06/18 PY - 2025 N1 - https://doi.org/10.11648/j.ijidt.20251002.12 DO - 10.11648/j.ijidt.20251002.12 T2 - International Journal of Infectious Diseases and Therapy JF - International Journal of Infectious Diseases and Therapy JO - International Journal of Infectious Diseases and Therapy SP - 39 EP - 46 PB - Science Publishing Group SN - 2578-966X UR - https://doi.org/10.11648/j.ijidt.20251002.12 AB - Acute respiratory infection (ARI) is a leading cause of morbidity and mortality in children in low and middle-income countries. Human metapneumovirus (HMPV) is a common virus associated with acute lower respiratory infections (ALRIs) in children. We aimed to estimate the global prevalence, hospital admissions, and clinical complications of HMPV-associated ALRI in children. Between 2005 and 2024, we estimated the global burden of human metapneumovirus-associated ALRIs in children from more than 30 studies. We included data for any length of study period. We included data on the proportion of HMPV-positive cases among hospitalized ALRI cases and patient attending outdoor wings with complain of severe or mild respiratory complications. According to estimates, HMPV caused 14.2 million ALRI cases in children under the age of five in 2018, which resulted in 643,000 hospital admissions and 7,700 in-hospital deaths. Children hospitalized with HMPV infection, as compared with those hospitalized without HMPV infection, were older and more likely to receive a diagnosis of pneumonia or asthma, to require supplemental oxygen, and to have a longer stay in the intensive care unit. Fever (97%) and cough (96%) were the most common presenting symptoms of HMPV-associated pneumonia and were also common symptoms of other pathogens. This study describes global prevalence and clinical complications of HMPV associated ALRIs in children. Clinical features did not reliably distinguish HMPV-associated ALRI from other respiratory infections. VL - 10 IS - 2 ER -
Department of Microbiology, Bangladesh University of Health Sciences, Dhaka, Bangladesh
Department of Microbiology, Bangladesh University of Health Sciences, Dhaka, Bangladesh
Department of Microbiology, United Medical College, Dhaka, Bangladesh
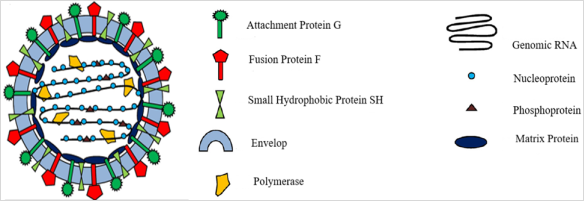
Figure 1. Schematic representation of HMPV and of hRSV viral particle [6].
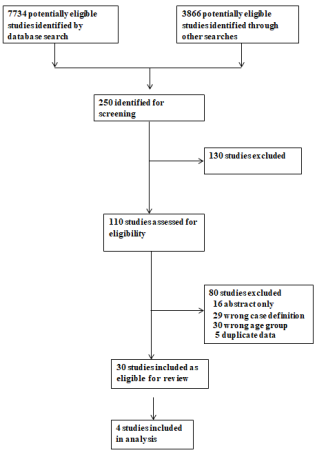
Figure 2. Study selection procedure.
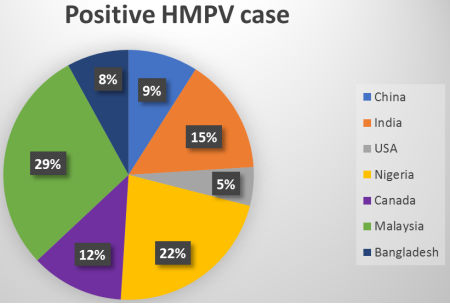
Figure 3. Pie chart shows the global prevalence of HMPV virus.
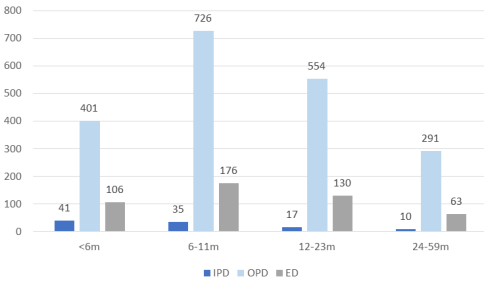
Figure 4. Rates of patients attending in IPD, OPD and ED for treatment of HMPV infection.
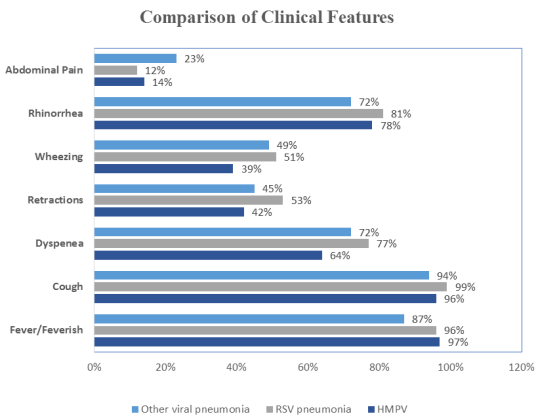
Figure 5. Clinical features of Hospitalized Children with HMPV Compared with RSV Pneumonia & Other Viral Pneumonia.

